
‘Bad’ Cholesterol May Not Be So Bad
Doctors say there are better alternatives to LDL cholesterol tests
By: Marina Zhang | The Epoch Times
For decades, low-density lipoprotein (LDL) cholesterol was one of the most critical indicators that doctors measured for heart disease. Now, doctors and researchers are challenging whether LDL cholesterol, also known as “bad cholesterol,” is really as bad as we once feared. Research shows that measuring LDL cholesterol doesn’t always effectively assess a person’s cardiovascular risk and that other tests may be more useful.
Low-Density Lipoproteins versus LDL Cholesterol
Many people with normal LDL cholesterol levels may experience heart attacks, cardiovascular research scientist James DiNicholantonio told The Epoch Times via email.
The number of LDL particles, rather than LDL cholesterol, may be a more relevant risk factor.
Studies have shown that LDL cholesterol levels predict higher cardiovascular risk 40% of the time, while apolipoprotein B (apoB) concentration, the summation of all LDL particles and their precursors, is associated with elevated risk 70% of the time.
Nourish The Heart & Blood Vessels With These 5 Foods, Plus 2 Cardioprotective Acupoints
Other studies comparing LDL cholesterol levels against cholesterol levels in LDL and its precursors, apoB number, and LDL particle number, also found that the latter two tend to be stronger predictors of risk, while LDL cholesterol is the weakest.
So what’s the difference between LDL particles and LDL cholesterol?
An LDL particle is a type of lipoprotein made by the liver. Its primary function is to deliver triglycerides from the liver to other cells in the body. Transporting cholesterol is more akin to an LDL’s side hustle. The cholesterol that an LDL transports is called LDL cholesterol.
High-density lipoprotein (HDL) and LDL cholesterols contain the same cholesterol; their carriers are what differ. LDL cholesterol can also leak into blood vessels, causing atherosclerosis, thereby earning its “bad” reputation.
On the other hand, HDL particles can venture into atherosclerotic plaques to absorb the cholesterol trapped inside, preventing further plaque formation and helping to prevent heart disease. Hence, HDL cholesterol is considered “good.”
Therefore, nutritionist Jonny Bowden says labelling HDL and LDL cholesterols as good and bad cholesterol is wrong.
Mr. Bowden, who co-authored the bestselling book “The Great Cholesterol Myth,” compared measuring the number of LDL particles to counting the number of passengers traveling in cars on a road. We know that more cars mean more congestion and traffic accidents, but more passengers doesn’t necessarily indicate this. Conversely, traffic could still be congested even if passenger numbers are low or average.
“My LDL [cholesterol] was like 100, maybe 110 mg/dL; very, very close to ideal,” Mr. Bowden said. “Then I got the particle tests, and they showed an entirely different picture.”
The test showed that he carried many small, dense LDL particles in his blood and was at high risk for cardiovascular events.
2 Types of LDL, 1 Is More Harmful
There are two types of LDL particles: large and buoyant, and small and dense.
The small and dense LDLs are much more atherogenic (contributive to atherosclerosis), whereas the large, buoyant LDLs are less so. These two types of LDLs can be measured through advanced lipid testing.
About 80% of total LDL cholesterol level comprises the more harmless large, buoyant LDLs, with atherogenic small, dense LDL making up the rest.
Interestingly, fats increase large, buoyant LDLs and decrease small, dense LDLs, whereas refined carbohydrates increase small, dense LDLs. Professor Erik Froyen from California State Polytechnic University, who has a doctorate in nutritional biology and whose research investigates mechanisms by which fatty acids impact cancer and cardiovascular disease risk factors, has also demonstrated this in his work.
Some research suggests that intake of refined carbohydrates is more relevant than saturated fat in causing coronary heart disease.
Mr. Bowden compares large, buoyant LDLs with large volleyballs that float along in the water, moving with the tide, while small, dense LDLs are like small golf balls that get stuck between rocks, where they start oxidizing and accumulating to form atherosclerotic plaques.
Individuals with more large, buoyant LDLs are said to exhibit a pattern A type of cholesterol profile, and these people are at low risk of atherosclerosis.
On the other hand, those with more small, dense LDLs exhibit a pattern B cholesterol profile and are at risk of atherosclerosis. Their markers for metabolic disease risks may also be elevated.
Small, dense LDLs carry less cholesterol than large, buoyant LDLs, so a person can have a normal LDL cholesterol level but a pattern B cholesterol profile.
However, lipidologist professor Carol Kirkpatrick, head of the Wellness Centre at Idaho State University, highlighted that for most people, overall LDL particle number is more relevant than LDL size.
“What we know now is that, yes, [small dense LDLs] may be important, but it really ends up being a red flag for people who have metabolic dysfunction,” Ms. Kirkpatrick, who is also a registered dietician nutritionist, told The Epoch Times.
Some studies have found that large LDLs have a neutral effect on atherosclerosis, though other scientists disagree.
“We know that statins, for instance, lower cardiovascular risk, and statins preferentially reduce larger LDL particles,” said Professor Kevin Maki of Indiana University, whose interest is in preventing and managing cardiometabolic disease.
However, the statin and LDL link has also been challenged.
“It’s really unclear if the benefit of statins is because it lowers LDL,” cardiologist Dr. Robert Dubroff told The Epoch Times.
“There are other drugs that can lower LDL, and many of them have been tested in well-conducted randomized trials and shown no benefit.”
Dr. Dubroff indicated that there are interventions that lower cardiovascular risk without lowering LDL.
Coronary Heart Disease: A Multifactorial Disease
Cardiovascular disease can be caused by various factors unrelated to LDL particles and LDL cholesterol.
Age is the most significant risk factor for cardiovascular disease, Mr. Maki said. The same is the case for one’s blood vessels and the blood vessels’ inner linings as he or she ages. Damage to the lining can result in inflammation, which raises LDL particle levels and may precipitate atherosclerosis.
Inflammation is also recognized as a risk factor, encouraging plaque formation and elevating LDLs in the bloodstream.
Insulin resistance is also increasingly recognized as a major contributor. It strongly correlates with Type 2 diabetes, which doubles the risk of death from heart disease or stroke.
Professor Benjamin Bikman from Brigham Young University told The Epoch Times that he sees two sides to insulin resistance: hyperinsulinemia, meaning high blood insulin, and actual insulin resistance, where the body no longer sufficiently responds to insulin.
Hyperinsulinemia encourages the formation of small, dense LDLs rather than large, buoyant ones. Insulin also increases blood pressure and encourages endothelial growth inside blood vessels, both related to atherosclerosis.
Dr. Dubroff said a patient who suffered multiple cardiovascular events was transferred to him a few years ago. The patient underwent coronary artery bypass three times and had been treated aggressively with statin medications, but his cardiovascular events continued.
Dr. Dubroff noticed that his patient’s blood sugar was borderline pre-diabetic and that he was overweight and had high blood triglycerides and low HDL. However, none of these risk factors were addressed by previous doctors.
He told his patient that the correct way forward was to improve his diet, lose weight, and exercise more.
Dr. Dubroff followed this patient for an additional 10 years.
“He never had any additional problems, even though his cholesterol level did not change,” Dr. Dubroff said.
Regarding tracing the source of one’s heart disease, Mr. Maki said: “I would say it’s not this or that, it’s this and that. LDL cholesterol is a factor; particle concentration is a factor; insulin resistance is a factor.”
Addressing all risk factors instead of one will enable us to be the “most successful at reducing cardiovascular risks,” he said.
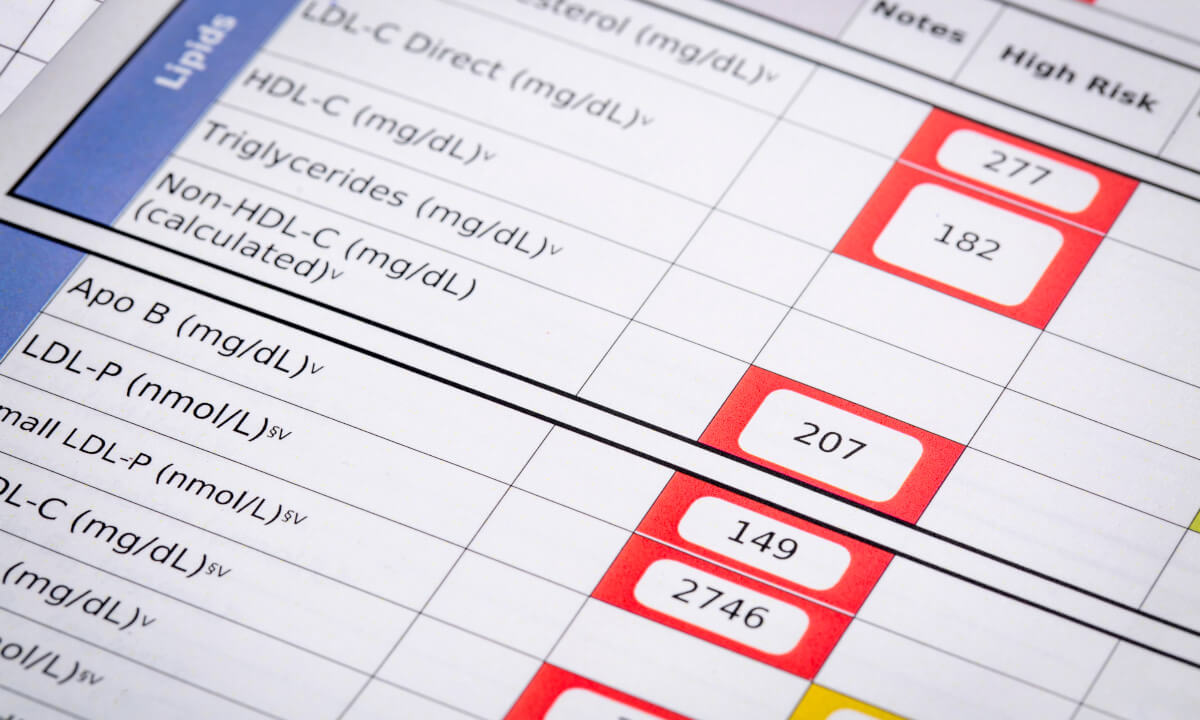
Better or Add-Value Tests
The advanced lipid test can better identify high-risk people with normal LDL cholesterol profiles. The test usually looks at LDL particle numbers or apoB numbers, which provide the total number of a person’s non-HDL lipoprotein particles.
Non-HDL particles include VLDL, IDL, and LDL particles. VLDL and IDL are precursors to LDL particles, so a high non-HDL particle number suggests high LDL particles.
However, advanced lipid testing usually isn’t covered by insurance. Therefore, health professionals sometimes offer alternative markers for examination.
Mr. Maki said that if he could only pick one thing to examine, he would choose non-HDL cholesterol, colloquially known as the “poor man’s apoB.”
This test is covered by insurance and looks at all the cholesterol carried in the non-HDL lipoproteins. While it provides a weaker predictive value than apoB, it can give a general indication of whether more particles are traveling in the bloodstream.
Mr. Bowden and Mr. Bikan suggested the triglyceride-to-HDL ratio to calculate insulin resistance.
When a person’s insulin levels are high, it encourages the destruction of HDL particles while encouraging blood triglyceride production. This leads to more LDL particles, especially small, dense, atherogenic LDL particles in the blood.
Markers for inflammation may also be suggestive of atherosclerosis. Inflammation can cause C-reactive protein (CRP) levels to become elevated. CRP can enter blood vessels and create an atherogenic environment.
* * *
NEXT UP!
Can A Dental Infection Cause A Massive Heart Attack?
For literally hundreds of years now, the idea that a dental infection could seed, initiate, and promote virtually all chronic degenerative diseases has been hotly debated in the medical and dental communities, often with much more passion and hyperbole than with science.
This “debate” continues today, and nothing encapsulates this focal infection link between the mouth and the body better than the root canal-treated tooth.
And while the root canal-treated tooth is certainly not the only significant source of dental infection and toxicity, it is easily the most devastating one—as you will soon see.
* * *
READ MORE: What To Eat To Defend Your Heart
Read more on LONGEVITY: Longevity Isn’t Really About Our Genes, Study Reveals
Liked it? Take a second to support Collective Spark.
We’d love to hear from you! If you have a comment about this article or if you have a tip for a future Collective Spark Story please let us know below in the comment section.