
The Man Who Saw The Future
If you're sceptical about the paranormal, the tale I'm about to share could completely change your perspective.
In May of 1921, after a sudden illness, a man named Paul Amadeus Dienach slipped into a mysterious coma that lasted an entire year.
But as bizarre as this sounds, it wasn’t the strangest thing that happened to Dienach.
When the young Swiss teacher finally came to, not only was he perfectly fine but he also seemed to have acquired a supernatural ability to predict the future.
I know this sounds so left field. But frankly, Dienach’s revelations after coming back from his coma are things that simply cannot be accounted for any other way.
He spoke of things like a hand-held box that brings pictures to life. In other words an iPad.
He also predicted quite a number of things that would happen a full century later like our attempts to colonize Mars, and even nuclear wars. And this was at a time when World War 2 hadn’t even happened yet.
If you don’t believe in the paranormal, then the story I’m about to tell you might just shatter your worldview. So, brace yourself. And if you do believe, well, you’re going to want to hear this.
* * *
NEXT UP!
USAF Flight Nurse Interviewed Alien Named Airl, Said Earth Was Alien Prison Before 30,000 BCE
All Aliens and UFO mysteries that have appeared in recent decades have been centred on the Roswell disaster. Officially, the extraterrestrial craft that landed in New Mexico in 1947 was never claimed, but many people claimed to have seen an alien ship on that day. There are dozens of reports claiming that aliens were recovered and possibly survived the crash. The administration will, without a doubt, constantly deny it. On the other hand, some people and officials accept the aliens’ rescue story and believe the UFO crash happened. According to excerpts from her notes and records, Matilda O’Donnell McElroy, Senior Master Sergeant Women’s Army Air Force Medical Corps, interviewed an alien named “Airl” who informed her where they came from and why they came to Earth.
Matilda was only 23 years old when she conducted a telepathic conversation with the alien. She was the only one in the base who could communicate with entities using her mind. She discovered during her discussion with Airl that the extraterrestrial was not a biological person, had a female-like appearance, and had not been damaged during the accident.

She described the extraterrestrial as being the size of a bit of child and the only survivor of the ship’s three crew members who had perished in the crash in New Mexico. Her body was composed of synthetic material, indicating that she was a higher-order being’s alien robot.
The UFO was made of the same material as the extraterrestrial body, according to the book “Alien Interview” (2008), which is based on Matilda O’Donnell McElroy’s notes and documented interviews. The mind and thoughts were in charge.
Video: Woman’s Encounter With Grey Aliens Reveals The Future of Our Planet
Lawrence R. Spencer, the book’s author, claimed to have received a letter from Matilda in which she revealed details concerning the series of conversations with Airl. She said that a species of aliens known as the Domain Expeditionary Force had been conducting operations in the solar system for 10,000 years, using the asteroid belt as an intergalactic base.
Matilda was assigned to the 509th Bomb Wing as a flight nurse. She asked Airl several questions about her civilization, star system, and history. According to their chart, the girl had come from a place called “Domain,” according to their conversation. As Matilda described it, that area was not just one galaxy’s planet but a galaxy’s worth of galaxies.
Her home (Birthplace), according to the alien, was full of power, knowledge, and wisdom. Her planet has three moons and two stars.
According to Matilda, the girl did not offer Matilda just about any information or the location of her planet. She was suspicious of military officers’ motives; thus, she refused to reveal any classified information to humans.
It was a dangerous sign, according to the nurse, since if aliens did not find a haven on Earth, it could become a significant problem for humanity. Air described her civilization as “very powerful,” “extremely ancient,” and “only concerned with progress.”
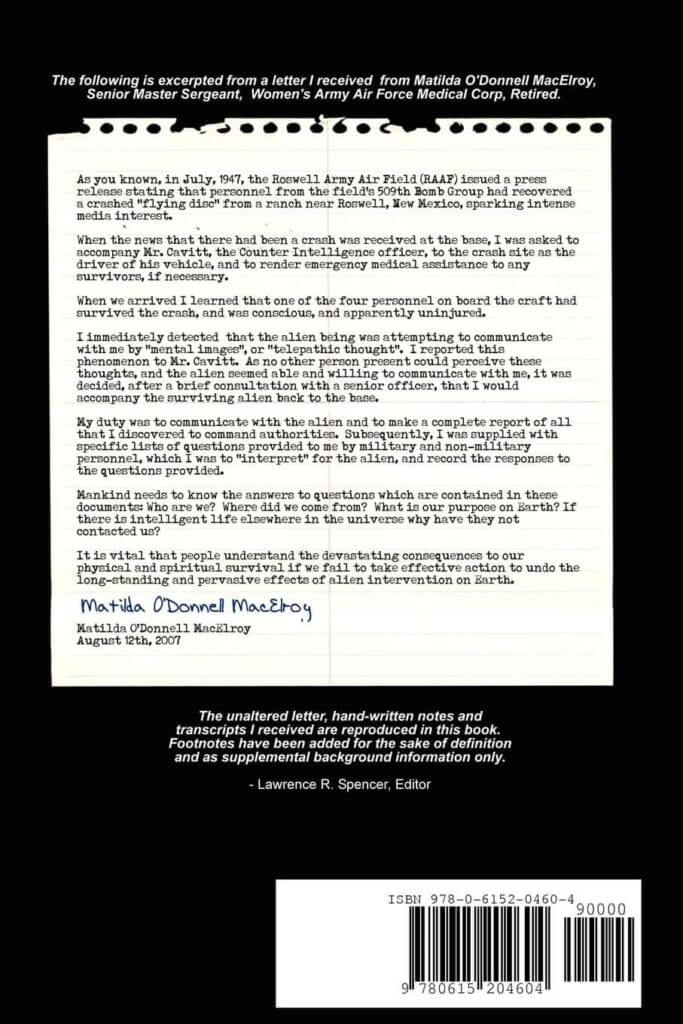
“Mankind needs to know the answers to questions that are contained in these texts,” MacElroy stated in the letter. Who are we, exactly? Where did we originate? What is the purpose of our being on this planet? Why hasn’t intelligent life from other parts of the cosmos contacted us? People must comprehend the dire ramifications for our bodily and spiritual survival if we do not take meaningful action to reverse the long-term and widespread impacts of alien activity on Earth.”
“LONG BEFORE HUMANS,” Airl replied when Matilda inquired how long she had been visiting Earth.
Matilda wrote in her footnotes:
“Earth is a small planet orbiting a galaxy’s rim star. It geographically isolates Earth from the more concentrated planetary civilizations that dwell toward the galaxy’s core. Because of these evident realities, Earth is only appropriate for use as a zoological or botanical garden or as a jail, as it is now.
Before 30,000 BCE, Earth was utilized as a landfill and prison for IS-BEs deemed untouchable, including criminals and non-conformists. IS-BEs were captured in various sections of the “Old Empire,” encased in electronic traps, and transferred to Earth. On Mars and Earth, Amnesia stations were placed underground. Africa’s Rwenzori Mountains, Portugal’s Pyrenees Mountains, and Mongolia’s steppes.”
Matilda’s story sounds like something out of a science fiction film, with her talking about interstellar adventures.
ESMA movies published a short CGI film called “The ex-Esma 2008” on YouTube in 2009, in which a deviant infant (alien) was converted into a human and deported to Earth by ETs after disturbing the peace on their planet.
The film is an odd notion, but it reminds me of Matilda’s description of Earth as a jail for I BEs who were thrown here and encased in electronic traps.
* * *
A Must Read TODAY!
Analysing The Leaked Video of An Alien Encounter (Video)
Back in 2017, a captivating video emerged, purportedly capturing a fascinating meeting between a human and what seems to be an Alien Grey at Area 51—an infamous and heavily speculated US military facility.
While the footage appears remarkably genuine, we must consider the possibility that it could be an artfully crafted CGI creation.
Area 51’s Alien Encounter: Real or CGI?
* * *
READ MORE: Retired US Army Officer Claimed Grey Aliens Are ‘Bio-Robots’ Built To Travel To Other Planets
Read more on The GREYs: Grey Aliens Are Created From Human DNA, Says Pennsylvania UFOlogist Professor
Telegram: Stay connected and get the latest updates by following us on Telegram!
We’d love to hear from you! If you have a comment about this article or if you have a tip for a future Collective Spark Story please let us know below in the comment section.
Is he for real what do you think?